
Ectopic Pregnancy
Mindy M. Horrow, MD, FACR, FSRU
Director of Body Imaging
Einstein Medical Center
Professor of Radiology
December 3, 2012
Clinical Features
Incidence: 1.5 -2% pregnancies, 15% all maternaldeaths and 80% of 1st trimester deaths
–Incidence in 1948 of 0.37%
-hCG – often rises at a slower rate and/or mayplateau, but 21% of ectopics have normal rising levels
Risk related to tubal abnormalities: previous EP, tubalsurgery, PID, IUD, increased maternal age and parity,prior C-section
Classical findings < 50%
–Pain, bleeding, adnexal mass
Lin, etal Radiographics 2008;28:1661
Diagnosis
★★Transvaginal ultrasound★★
No reliable serum markers
Screening not thought to be cost effective
–With possible exception of prior tubal ligation
Progesterone: primarily an indication of viabilityrather than location.
–> 25 ng/ml has 98% association with normal IUP
–< 5 ng/ml indicates non-viable pregnancy regardless oflocation
–Most ectopic pregnancies have progesterone levelsbetween these two concentrations, limiting the usefulnessof this measurement
Sowter, Curr Opin Ob Gyn 2004;16:289
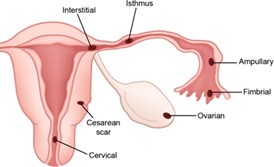
Location
Fallopian tube
–Ampullary- isthmic - 95%
–Interstitial (cornual) – 2 -3% (intramural portion oftube where it passesthrough wall of uterus toenter endometrial canal)
Extra-tubal: RARE
–Abdominal, cervical,uterine scar, ovarian
Sonography: Technique
Initial transabdominal view to look foradvanced IUP, large mass or largeamount of fluid/blood
Transvaginal
± Doppler
Sonography of Ectopic Pregnancy
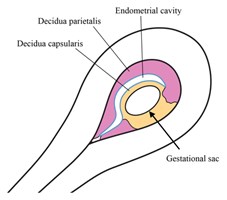
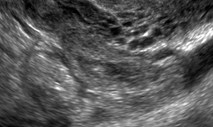
Endometrium
Adnexa
Free fluid
Doppler
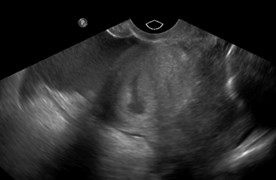
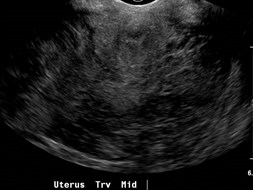
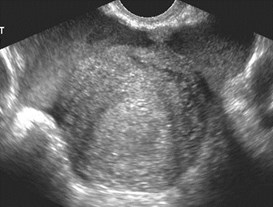
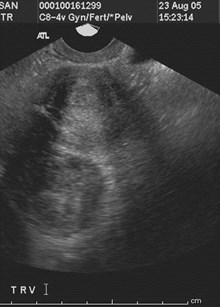
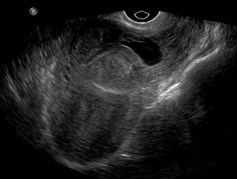
Endometrium
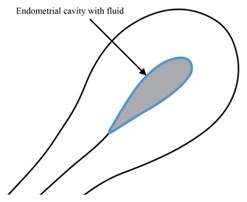
Pseudosac-
–Fluid collection, often blood in endometrial cavity
–Occurs in up to 20%
Decidual cysts
Appearance and thickness of endometrium: not veryuseful
–EMS usually thinner in patients with EP compared to normalIUP and spontaneous AB, because of lower -HCG levels
–Thin, tri-laminar EMS is specific (85 – 94%), but not verysensitive (10-38%) for EP
Hammoud, AJOG 2005;192:1370
Wachsberg J Clin US 1998;26:199
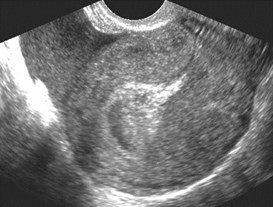
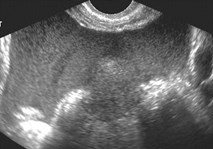
Examples of pseudosacs

Usually multiple, located at endometrialmyometrial junction, thin walled comparedto gestational sac

Examples of decidual cysts

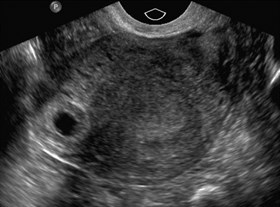
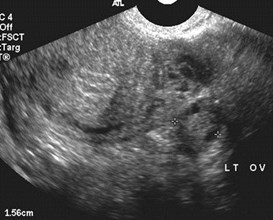
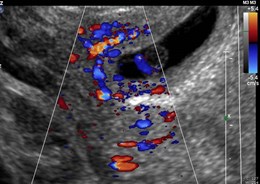
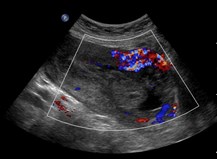
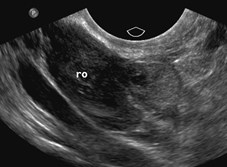
Adnexa
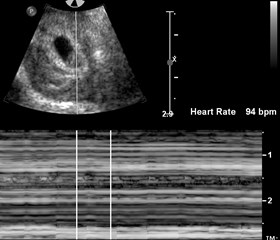
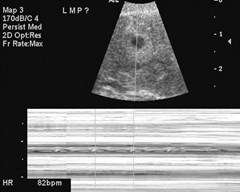
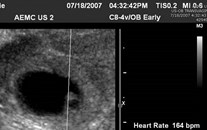
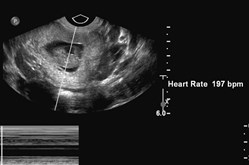
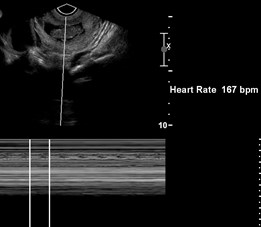
Live ectopic pregnancy
Non-viable ectopic pregnancy
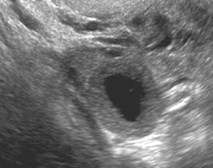
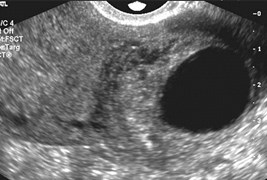
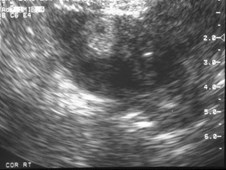
Tubal ring
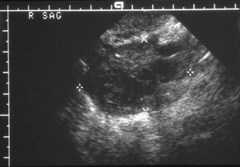
Hematosalpinx: “mass” or“blob” separate from ovary
Study of 200 patients with surgically provenectopic pregnancy and pre-operativetransvaginal scan
57.9 % inhomogeneous blob or mass
13.2 % with embryo cardiac activity
20.4 % hyperechoic ring in adnexa
7.2 % no IUP or ectopic visualized
1.3% heterotopic pregnancies
Sen 90.9%, Spe 99.9%, PPV 93.5%, NPV 99.8% for TVUS todetect the ectopic pregnancy
Condous Human Reprod2005;20:1404
Highly dependent on quality of scanning


Small tubal rings


Transvaginal more limited than transabdominal imaging


If scanning TA, try higher frequency transducer

Examples of hematosalpinges


Hematosalpinx with identifiable tubal ring

Hematosalpinx containing live ectopic
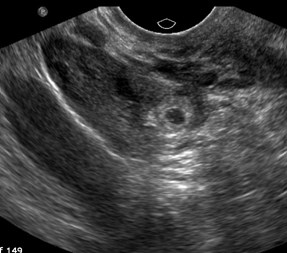
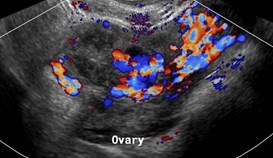
Tubal “Ring” vs. CorpusLuteum
Corpus luteal cyst is eccentric with rim of ovariantissue
Tubal ring has concentric echogenic rim and is oftensurrounded by a hematosalpinx
Echogenicity of tubal ring greater than ovarywhereas corpus luteal cyst is equal to or lessechogenic.
When a corpus luteum was visualized, 80% hadipsilateral ectopic pregnancy
Anechoic or complex ovarian cyst most likely acorpus luteum because ovarian ectopics are < 1%of all ectopic pregnancies
Frates, JUM 2001;20:27
Condous, Human Reprod 2005;20:1404

Corpus luteum versus ectopic tubal ring

Right Interstitial (Cornual) Ectopic
Interstitial Ectopic Pregnancy
Because of intramural location, rupture may belater than usual EP, but cause massivehemorrhage with higher mortality.
Myometrial thinning and sac eccentricity notalways reliable
“Interstitial line sign” – a thin echogenic linefrom EMS to cornual sac or echogenic massseen in 92%
Treatment: laparotomy with cornual resection,methotrexate (local or systemic)
Ackerman, Rad 1993;189:83

Trans-abdominal view
Trans-vaginal views

Non-viable interstitialectopic pregnancy
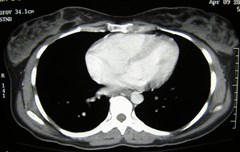
Free Fluid
Pelvic and abdominal
If complex, indicates hemoperitoneum
Presence or absence of fluid does not necessarilyindicate rupture (Significant bleeding can occurfrom fimbriated end of tube, without rupture)
Transvaginal sonography has virtually replacedculdocentesis
Small amounts of simple fluid are physiologic
Frates, Rad 1994;191:769

Ruptured ectopic, clotted bloodobscures uterine borders


Ruptured ectopic, large amount of bloodbetter appreciated transabdominally
If clinically unstable, can terminate examwithout demonstrating ectopic pregnancy
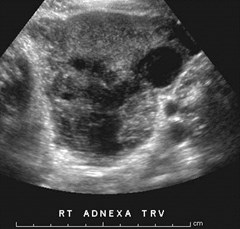
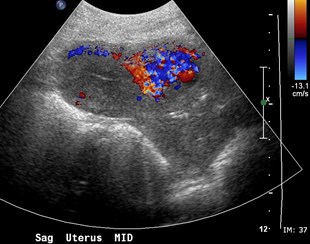
Sagittal Transverse
R Adnexa: Transverse Sagittal
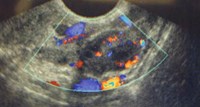
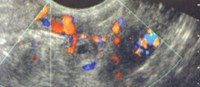
Ruptured Right Ectopic Pregnancy
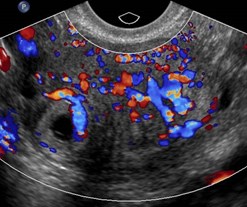
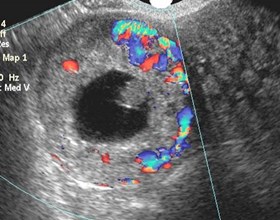
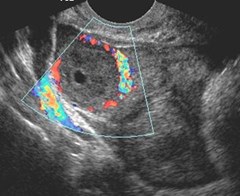
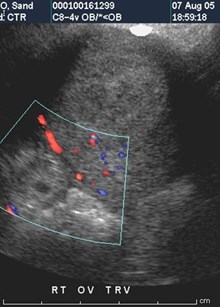
Color Doppler helps locate EP



-HCG 890

Images of “Mass” in cul-de-sac
At surgery fallopian tube was intact,with EP aborted into cul-de-sac



Acute pain, - HCG 22
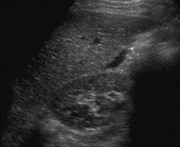
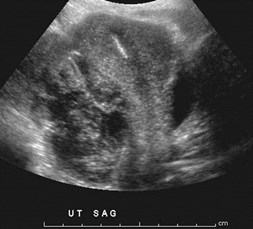
Ruptured left ectopic pregnancy



Sent by ER and OB to confirmdemise
Where is uterus?
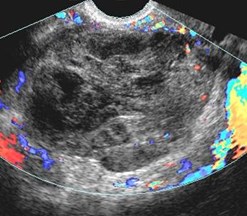
Ruptured ectopicpregnancy
42 yo with acute pain and hypotension
Acutely bleeding, ruptured EP
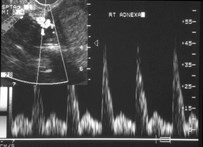
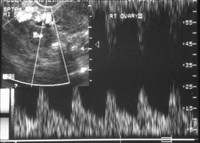
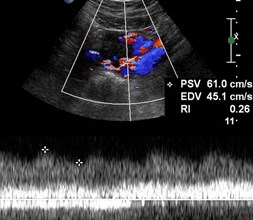
Doppler Analysis
Low impedance placental(trophoblastic) flow
–Extrauterine
–Corpus luteal
Bizarre waveforms: very high andvery low resistive indices
Use of color Doppler slightlyincreases ability to detect the EP
Atri. JUM 2003;22:1181


Left-Transverse
Left Sag
Left ectopic pregnancy
Left corpus luteum
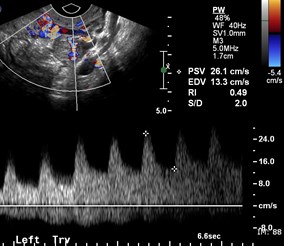
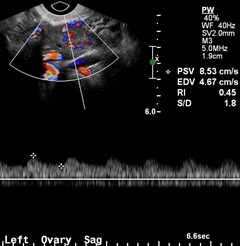
Similar low resistance flow in corpusluteum and ectopic pregnancy

7mm “donut” separate
from left ovary
L corpus luteal flow
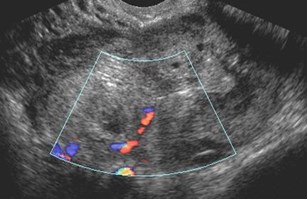
Flow in “mass” near ovary
7mm left ectopic
Color Doppler aids
visualization
Value of Doppler
Presence of extra-uterine trophoblastic flowhas sensitivity of 48% for EP
Doppler has lower sensitivity and NPV than2D imaging.
May have benefit for directing therapy. Ifvascular, surgery or medical therapyindicated. If avascular with dropping HCGlevels, ectopic tissue is being aborted.
Hypervascular ring of low resistance flow more likelyindicates corpus luteum than ectopic pregnancy
Management of Ectopic Pregnancy
Surgery- usually laparoscopy with eithersalpingotomy or salpingectomy
Spontaneous resolution- more common forstable patients with declining -HCG.Success rates near 70% in select group
Medical - methotrexate
Yao, Fertil Steril 1997;67:421
Methotrexate Therapy
Systemic vs. local
hCG levels at presentation predictoutcomes: 92.5% success if hCG < 4000IU/l
Criteria:
1. Stable patient
2. Growing EP ( -hCG)
3. No findings of rupture
4. EP < 3.5 cm
Stovall, Am J Obstet Gyn 1993
Tawfiq, Fertl Steril 2000; 74:877
Gamzu, Fertl Steril 2002; 77:761
Methotrexate vs. Surgery
Saraj, etal Ob Gynec 1998; 92:989
–78% success single dose methotrexate
–92% success laparoscopic surgery
Sowter, etal BJOG 2001; 108:192
–65% success single dose methotrexate
–93% success laparoscopic surgery
Sowter, etal BJOG 2001; 108:204
–Medical treatment associated with reduced directand indirect costs although at hCG levels > 1500IU/l benefits were lost due to need for prolongedfollow-up and surgical intervention
Methotrexate Therapy
Sonography
–Initially may increase in size or vascularity, free fluid.
–May take as long as 5 months for EPresolution
–Rupture may occur, causing pelvic pain and ahemorrhagic mass on sonography.
Atri et al, Radiology 1993

Pregnant patient with right sided pain and prior left
Salpingectomy for ectopic pregnancy
Dx: Right Ectopic
Pregnancy (2/23)
Treatment: Methotrexate
3/2 tubal ring visible 3/16 smaller
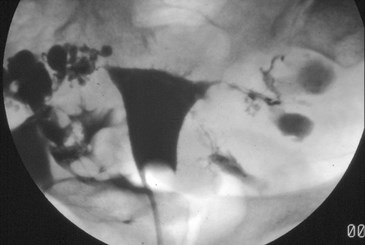
6 months later- hysterosalpingogram
Free spill right tube
Increasing size of tubal “mass”with methotrexate therapy

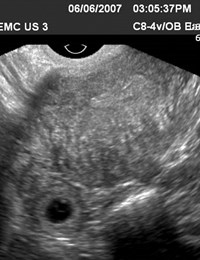
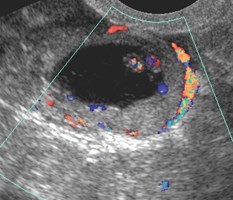
Right ectopic pregnancy treated with methotrexate on6-6-07, returns with pain on 7-3-07


Increased size of ectopic pregnancy, leakingblood, required surgery
Failed methotrexate
Other Issues
Unusually located ectopic pregnancy
Uterine and adnexal abnormalities
Ectopic pregnancy mimics
Advanced ectopic pregnancy mistaken forintrauterine pregnancy
Chronic Ectopic Pregnancy
Heterotopic pregnancy: high risk patients (IVF)or IUP with suspicious mass

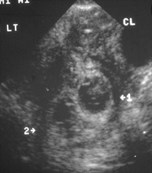
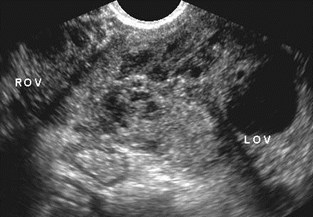
R OV

Mono-mono twin ectopic pregnancy


Diamniotic dichorionicTwin ectopic pregnancy
Stable pregnant patient with slight bleeding
Chronic Ruptured EctopicPregnancy

Had D&C after “miscarriage”, persistent spotting, -HCGstill positive, left pelvic pain
Chronic EctopicPregnancy
Chronic Ectopic Pregnancy
Repeated small ruptures cause hematoceleconsisting of clots, gestational tissue, adhesions
Surgery often difficult 2° adhesions
Patients often mildly symptomatic, sometimes withlonger duration of symptoms
Study of 305 EPS, found 20.3% (62) cases whichfit this description, 5 with negative -HCG (Uqur)
Bedi Eur J Radiol 1987;7:46
Uqur Aust NZ J Ob Gyn 1996;36:186



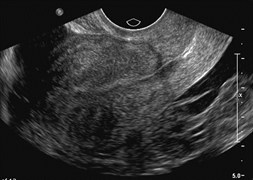
ER scan shows “ectopic pregnancy”
6.5 weeks IUP displacedby large fibroid



Live pregnancy growingin C-section scar

2 days later after systemic methotrexate
Surgery required to treat ectopicpregnancy
Caesarean Scar Implantation
Appears to be increasing in incidence
–5% of ectopic pregnancies in women with at least oneprior Caesarian section
History of painless vaginal bleeding and priorcaesarian section(s)
Pregnancy cannot continue because trophoblast willextend beyond uterus to bladder resulting incatastrophic hemorrhage and need for hysterectomy
May have similar appearance to an abortinggestational sac in the lower uterine segment, checkvascularity.
Jurkovic, US Ob Gynec 2003;21:220
Caesarean Scar Implantation
Gestation is completely surrounded by myometriumand fibrous scar and separate from endometrial cavityor fallopian tube
Probable mechanism is invasion of myometriumthrough a microscopic tract. Similar to interstitialpregnancy.
US Findings: empty uterine cavity, empty cervicalcanal, sac in anterior lower uterus
No consensus on treatment: Can try medical therapy,but only surgery will allow removal of the pregnancyand repair of the defect
Fylstra, Obstet Gyn Survey 2002;57:537
Pregnant patient with
Bleeding, 4-30

Interpreted asspontaneous abortionin progress

Still bleeding 6-06
Retained products ofconception of scar ectopic
Abortion in progress or ectopic pregnancy?



Patient A
Patient B



Live Cervical Ectopic Pregnancy
Patient B 10 days later
Cervical Ectopic Pregnancy
Occurs in 0.15% of all ectopic pregnancies
If sac is within endocervical canal and embryodemonstrates cardiac activity and/or trophoblasticflow, more likely a cervical ectopic than an abortionin progress
Surgery may lead to significant hemorrhage soconservative treatments include: US guided localinjection methotrexate or KCl or preoperative uterineartery embolization before dilation and evacuation
Levine Radiology 2007;245:385


Right Sag
Right Trv
Right pelvic pain in pregnancy conceived with Clomid
Heterotopic Pregnancy
Heterotopic Pregnancy: combined intraand extrauterine pregnancies
Risk ranges from 1 in 30,000 to 1 in 2100
In patients undergoing ovulation induction, risk maybe as high as 1% – 3%
Significantly higher risk in pregnancy assistedpatients due to frequent tubal damage and use ofsuperovulation and multiple embryo transfers
Accuracy of Sonography inDiagnosis of Ectopic Pregnancy
Reported sensitivities range fromapproximately 50% to 89-100%
Brown etal (JUM 1994; 13:259)
–If no IUP and an adnexal mass (except a simplecyst or intraovarian lesion): 84.4% sen,98.9% spec, 96.3% PPV, 94.8% NPV
Condous etal (Hum Reprod 2005; 20: 1404)
–90.0% Sen, 99.9% SPEC, 93.5 PPV, 99.8% NPV
When does ectopic pregnancybecome symptomatic?
Tubal: 5 - 6 weeks after LMP
Interstitial: 8 – 10 weeks after LMP
Abdominal: May present in 2nd or 3rd trimester
However patient may not rememberLMP or may have had bleeding relatedto ectopic
If the -hCG is positive US may show:
1. Intrauterine pregnancy (IUP) (normal, abnormal)
2. Extrauterine pregnancy
3. Presumed tubal pregnancy (tubal mass)
4. No IUP or tubal mass:Pregnancy of Unknown Location
Do NOT wait for Quantitative βHCG
THE END

King’s Canyon National Park 8-07